Back in the early 1990s, I first read about reflexology from one of my mom’s Hong Kong tabloid magazines. The cover photo depicted a “map” of the feet in Chinese, indicating that pressure upon a specific area on the foot or toes can ease pain or “promote healing” to certain internal organs. The narrative sounds a lot like acupuncture, which led me to believe that reflexology came from China. However, having dug into the evidence and history about reflexology, it seems that other civilizations and cultures had some concept of easing pain with foot and hand massage. While having pressure applied to the feet and hands feels good for most people, how accurate and reliable are the claims behind reflexology?
History of reflexology
Egyptian origins
One of the earliest evidence on foot massage as a health treatment is found in the Tomb of Ankhmahor in Saqqara, Egypt, around 2,300 B.C., which is cited by numerous reflexology textbooks. One website claims that the evidence of foot massage goes as far back as the late 25th century B.C. during the reign of Ptahhotep, where the vizier is depicted having a manicure and pedicure and having his legs massaged by a servant.
According to Egyptologist Engy El-Kilany from Minia University in Egypt, no one really knows for sure what these images actually depict. She wrote in the Journal of Faculty of Tourism and Hotels, “…there is still great debate regarding the nature of the therapy being depicted: is it surgery, reflexology, massage or simply manicure and pedicure?” (All images described by El-Kilany are in the journal’s link.)
She cited five scholars from the 1940s to the 1990s that the depiction is more likely to be a reflexology treatment rather than simply keeping the hands and feet clean. Evidence came from the accompanying texts with the images. In the tomb of Ankhmahor, El-Kilany described the scene:
“On the left, the practitioner handles the thumb of the client who says Do this, Put strength. On the right the practitioner handles the toe of the client who says Do not cause pain to this. The answer of both practitioners is written between them and it is the same I will do this as you wish, sovereign. Both clients put one hand under the shoulder and the other hand over the knee.”
The second scene described came from the tomb of Khentika where the vizier was depicted getting a pedicure and a manicure. Again, the hieroglyphs describes the scene as a “medical massage on the hands and feet.”
“It shows three men sitting on the floor. The client is squatting between two masseurs. The masseur to the right side is massaging the toes of the right leg of the client while the masseur to the left side is rubbing the fingers of the left arm of the same client. The written text mentioned ‘inspector of the treasury, Heny, Do it to please me Mery, I shall do it to please you’,” El-Kilany wrote.
Chinese origins
The Chinese culture seems to get most of the credit about the origin of reflexology. Perhaps it is the spread of traditional Chinese medicine (TCM) worldwide since the 1970s that fueled such belief, overtaking most of the other cultures’ narratives.
In TCM belief, there are 12 primary meridians that connect the hands and feet to the body, where six of them are from the hands and the other six are from the feet. These meridians are said to channel life-energy—known as “qi” (氣)—to the entire body. These meridians correspond to a primary internal organ, which are divided into six “Yangs” (陽) and six “Yins” (陰).
For the feet, the Yin meridians correspond to the liver, kidney, and spleen, while the Yang meridians correspond to the gall bladder, bladder, and stomach. It is believed that putting pressure upon specific points on the foot can “unblock” these energy channels, which can inhibit healing and health maintenance of an organ.
Native Americans origins
Some reflexology textbooks mention that Native Americans, such as the Cherokees, Incans, and Mayans had their version of reflexology. However, there is no solid evidence that they had ideas like modern reflexology during the pre-Columbian period. It is likely that various Native American cultures had use massage—including the foot and hand—as part of their folk treatments. Being human, it is also likely that massage is a form of social grooming and bonding, similar to most primates. Thus, it would be not much of a surprise if there is some kind of archaeological evidence that show many indigenous people worldwide use or had used massage therapy and touch as a way to ease another’s pain.
It is unlikely that the ancient Egyptians had a concept of a foot map that you often see in a reflexology chart. There is also no evidence that there was any contact between ancient Egypt (Old Kingdom Period to the Late Period) and ancient China (Xia to Zhou dynasties), considering the vast distance between both civilizations. Thus, it is likely that each culture independently developed an idea that hand and foot massages somehow had health benefits, similar to the some inventions were developed independently, like the bow and arrow, spear, and the pyramids (e.g. Aztecs vs. Egyptians)—the concept of “multiple discovery.”
Modern reflexology
Modern reflexology, at least in the U.S., Canada, and some European countries, likely had started with the work of Dr. William Fitzgerald (1872-1942), who was an American physician in Hartford, Connecticut. This is cited in multiple reflexology textbooks, such as those by Susan Cressy, Beryl Crane, and Adams Media. After practicing in Boston, London (England), and Vienna, he went back to practice in Boston some time in the late 1900s or early 1910s, where he eventually became the head of the nose and throat department of St. Francis Hospital in Hartford.
During this time, he found that by applying pressure upon certain areas of the feet, other places in the face and jaw become anesthetized. This allowed him to perform minor surgeries on the mouth, nose, and face without relying on morphine, cocaine, and other narcotics.
He divided each foot into five longitudinal “zones” which are numbered 1 to 5, starting with the big toe’s side as Zone 1. This zone supposedly can anesthetize the incisors and cuspids, while Zone 2 corresponds to the bicuspids, Zone 3 to the molars, and Zone 4 and 5 to the head (no specific areas were mentioned). The zones connect to the rest of the body through “ten invisible currents of energy.”
Almost all references to Dr. Fitzgerald’s work and biography come from reflexology and practitioners’ websites with very little references from academic journals. Another source of his work can be found in his 1917 book, “Zone Therapy,” which has gone several versions in the 20th century.
Fitzgerald never mentioned anything about how he got the idea of zone therapy nor did he reference his work to Asian or Egyptian origins. However, Crane said that his reflex areas correlate with most acupoints.
Other people continued with the concept of reflexology after Fitzgerald, including Eunice Ingham, her nephew Dwight Byers, Doreen Bayly, Mildred Carter, and Hanne Marquardt in the late 20th century.
How does reflexology work?
Acupoints & meridians
Whether they are called meridians, energy channels, or acupoints, these are some of the common things that attribute to the healing properties of reflexology, but do they exist?
Crane states that the touch from a reflexologist can “create a flow of energy” between a reflexologist’s hand and the patient’s body, which can “calm” and “relax” the patient. “Life energy can mean many different things to people working in different traditions,” she wrote. “Perhaps we should not try to explain it, but be satisfied with being aware of its existence. We should also keep in mind that we not only touch tissue, muscle and bone, but we also ‘touch’ the very life force of the body.”
However, these claims—like most of claims by energy medicine proponents—are not grounded in the fundamentals of our understanding of how energy works, which are the basis of understanding biology and chemistry, including our own physiology and biomechanics. Also, there has been no solid evidence of the existence of such acupoints and meridians that are supposed to channel throughout our body.
Some proponents say that the meridians follow very closely to our nerve system, and acupoints are found along vascular nerve bundles. One recent study published in Evidence-based Complementary and Alternative Medicine found these bundles exist near the meridians and outside of the imaginary lines. “The histology showed that, between verum (acupuncture meridian) and placebo, there is no detectable difference,” the authors wrote.
“Since we found [vascular nerve bundles] in just a few of the acupuncture points and as we found [vascular nerve bundles] even without an acupuncture point, we are no longer convinced that the sole concept of the function of the acupuncture system over neural reflexes is valid.”
Instead of nerves, the authors suggested that the superficial layers of fascia, “trigger points,”and parts of ligaments, tendons, and muscles “follow the meridian course.” Still, no one really knows whether these meridians actually exist or if the researchers are looking for patterns amidst the noise.
Toxins
“Toxins” and “detox” are commons words that you might often hear about the benefits of getting a massage, and such claims are not that much different with reflexology. Cressy wrote one of the benefits of reflexology is that it “detoxifies the body,” but she does not specifically say what kind of toxins are there nor does she explain how applying pressure upon the foot can remove toxins from the body. She also wrote that reflexology can improve the function of the lymphatic system and the skin in “excreting wastes.”
These claims, however, do not reflect on how the lymphatic system or pretty much how human physiology works. In fact, exercise and regular movement can help the lymphatic system pump the lymph fluid with consistent muscle contractions.

Biopsychosocial model of health
A more plausible explanation behind how reflexology works is based on the current pain theories, such as the gate control theory and neuromatrix theory of pain. These are based on the biopsychosocial model of pain where various factors (biological, psychological, sociological) create our unique pain experience.
More specific explanations about the analgesic effect would include descending modulation, distraction, and the placebo effect. Vigotsky and Bruhns compared the effects of various manual therapies, including massage, spinal manipulation, and neural mobilization. With the exception of getting the back cracked, all other interventions show some neurological and endocrinal effects on pain modulation.
While modern pain science can help reveal more plausible mechanisms of how reflexology works, these do not explain or validate Fitzgerald’s observations and claims about the anesthetic effects of pressure points on the foot correlating to certain parts of the face and head.
So is reflexology real?
If you ask if the relaxing and temporary analgesic effects of reflexology is real, then there is very little doubt that it is. Getting your feet rubbed and touched—coupled with a relationship with another person (the therapist) and your expectations of its healing effects—has similar effects to getting your back and neck massaged.
There is also plenty of research that examine the effects of reflexology on digestive effects, pain relief, and other ailments. It would be beyond the scope of this article to cover all the major research, but a few systematic reviews and trials are worth taking a peek.
Pain Relief
A 2012 Cochrane Review examined the literature behind the effectiveness of massage therapy and reflexology for pain management during women’s labor. The researchers included trials that are randomized-controlled and its subjects are women in labor—including those who are at high risk, such as those in preterm labor. What they were looking for were primarily how much pain the women had after the treatment, how much sense of control they had, and were they satisfied with the pain relief and childbirth experience.
While the researchers did not find any reflexology trials that qualify for their review, they found six qualified massage trials with a total of 326 women where the intervention was compared to “standard care.” Basically, they found that massage therapy was quite effective in decreasing pain in the first stage of labor, but there were many problems with these trials.
These problems include poor reporting in all trials, such as explaining how the massage was done and how the blinding was conducted, different methodologies which makes assessment of the review difficult, limited number of trials, and lack of consistency of pain reduction on all subjects.
Like many massage research, when you compare one group who gets a massage versus another group who doesn’t get one—and the people in the second group knows that they aren’t getting any—the first group would report feeling much better than before the experiment, and the second group would likely report feeling a little worse. You could call this a “frustrebo” effect where an intervention appears to “work” much better in the experimental compared to the control group, but in reality, it is likely the negative side effect of the control group of not receiving the treatment that exaggerates the benefits of the experimental group.
Keep this in mind when you read massage and other manual therapy research.
See Placebo Power Hype for details.
Constipation
A 2009 Cochrane Review examined whether reflexology could reduce the symptoms of chronic constipation. However, only the protocol was published and it seems that the systematic review was never conducted.
An observational trial in 2003 examined 50 children between ages three to fourteen who were diagnosed with encopresis and chronic constipation. They had six 30-minute sessions of reflexology over a six-week period at an undisclosed outpatient clinic. Overall, the subjects went from an average rate of 78 percent of soiling once a day to 20 percent, 16 percent of soiling one to three times a week to 30 percent, and six percent of no soiling to 48 percent.
For constipation, those with no bowel movements for a week went from 36 percent to 2 percent, one to four bowel movements from 46 percent to 72 percent, and daily bowel movements from 18 percent to 24 percent.
The problem with this trial there is no control group, so we do not have a comparison of whether a regular foot massage or just having a “social visit” by a caregiver would have a similar or different effect. Also, no effect size was reported so we don’t really know for sure if this is clinically significant.
Two recent randomized-controlled trials were done on the elderly, including one study from Ankara, Turkey, and the other from Arak, Iran. Both of them found effectiveness of reflexology for increasing daily and weekly bowel movements. However, there are a few issues with these studies.
With a sample size of 60 people, the Turkish study compared reflexology to a foot massage that did not include the application of pressure points. The 30-minute treatment was done three times a week for a month in the morning after the subjects had breakfast. Before the experiment, both groups had similar rates of bowel movement (63.3% experimental, 65.5% control), but the researchers did not say at what rate.
At the end of the month, 20 percent of the experimental group and 72 percent of the control group had a bowel movement every three days. None of the experimental group and nearly 21 percent of the control group had a bowel movement every four or more days.
While both groups show some improvements of constipation, there were more people from the control group with improved bowel movements every three days than the experimental group. Even though none of the experimental group had a lack of bowel movement every four or more days, how could the authors justify reflexology had “considerably higher increase in bowel movement frequency in our experimental group” when a foot massage had similar improvements?
Like the pediatric study, would offering a social visit with a massage three times a week for a month improve the symptoms of constipation? Were there other confounding factors in the people’s life that may have affected their improvements?
In the Iranian study, 63 patients with constipation and multiple sclerosis participated in the double-blinded, randomized-controlled trial that lasted six weeks with two 30- to 40-minute treatments per week. The set up was similar to the Turkish study where the experimental group received reflexology while the control received a foot massage without pressure points.
At the beginning of the study, both groups had similar bowel movement rates of every four days. At the end of the study, the experimental group’s rate dropped to every 2.5 days while the control group remained almost unchanged. There was no difference in the quality of life between the groups, the authors reported.
Given the number of trials that has been done since the 2009 Cochrane protocol was made, perhaps a systematic review would shed some light on the quality of these studies.
Breast cancer symptoms
A 2010 South Korean systematic review examined four qualified trials on the effects of reflexology on breast cancer patients’ symptoms, such as vomiting and nausea. This review included one randomized-controlled trial from the U.K. and three non-randomized-controlled ones from South Korea. They found the U.K. study had a low risk of bias while the South Korean ones had a high risk bias, which could lead to “false positives” to their positive outcomes. “…the evidence was inconclusive that reflexology was more effective than [self-initiated support] or no-treatment (as an add-on to conventional oncologic treatment or chemotherapy),” the authors wrote.
Although the U.K. trial had a low risk of bias and a positive outcome, the authors indicated that its methodology (A + B vs. B) cannot “was unable to demonstrate specific therapeutic effects of reflexology.” For the other three studies with also positive outcomes, they said that selection bias could influence the results.
Limitations include “small sample sizes, inadequate control for nonspecific effects, a lack of power calculations, and short follow-up or treatment periods.” In one of the effect size, an anti-emetic drug was used to control vomiting, so there the researchers could not further identify reflexology’s specific effects.
The systematic review itself, however, is still limited because of the low number of studies, overall high risk of bias in the trials, publication bias, and using mostly Korean databases. Thus, based on the current evidence the authors said that “reflexology could not be used for improvement of the symptoms including pain, nausea and vomiting, and mood disturbances of patients with breast cancer.” They suggested that patients who are using or considering this treatment should be provided with the current evidence, thus being informed and provided consent.
Children and teens
Using the Cochrane Review guidelines, a 2020 systematic review from Antalya, Turkey, examined six qualified randomized-controlled trials that included infants to 18-year-olds. The researchers included the effects of reflexology on constipation, colic, acute pain, neonatal abstinence syndrome, spasticity and motor function in cerebral palsy. All but one (Iran) were Turkish studies.
While most of the studies had reported positive outcomes, the risk of bias was high among the cerebral palsy, colic, and constipation studies. Like the previous systematic reviews, the low number of trials, high risk of bias, miss reports of how the method was done, and language bias make it difficult for the researchers to make draw any solid conclusions.
However, the researchers in this review seem to support reflexology as a method of treatment: “Reflexology reflects the body like a mirror, and it responds quickly to stimulation. It is a useful practice for children in terms of both efficacy and simplicity of application.”
They recognize that touch by nurses and caregivers do promote better health for infants and children, but there was no mention of biopsychosocial effects (other than placebo among older children) that were likely to influence some of the outcomes.
Largest number of trials reviewed
While most systematic reviews that target specific problems that reflexology could aid have a low number of studies, the largest one to date consists of 23 randomized-controlled trials that examined reflexology for different ailments, such as asthma, headache, cancer palliation, menstrual pain, low back pain, and post-cholecystectomy. Conducted by Ernst et al. in 2010, these trials include 14 with negative outcomes, eight positives, and one unknown. Like most reflexology trials reported in other reviews, many of these trials have poor methods, lack of quality control of non-specific effects, and lack of independent replications.
Because of biological implausibility, publication bias against negative studies, and poor quality of existing studies—and potential frustrebo effect—claims behind reflexology should be taken with a grain of salt.
Outcomes measures do not validate reflexology
The results of an experiment does not automatically validate that an intervention works because clinical outcomes are influenced by many factors, such as the natural course of a disease or pain, placebo effects, regression to the mean, and physical and social environmental factors.
Reflexology, massage therapy, and other forms of touch are just one factor among many that influences patients’ perception and expectation of their health experience and the intervention given. This is why we need high-quality randomized-controlled trials to give us any degree of certainty for how good or poor an intervention is.
“A good outcome does not necessarily indicate that intervention was effective; the good outcome may have occurred even without intervention. And a poor outcome does not necessarily indicate that intervention was ineffective; the outcome may have been worse still without intervention….It is illogical, on the one hand, to look to randomised controlled trials for evidence of effects of interventions while, on the other hand, seeking justification for the effectiveness of clinical practice with uncontrolled measurement of clinical outcomes.” ~ Herbert et al. (2005)
There are also a few things to consider when reading a research about reflexology or any other interventions.
Positive studies and publication bias
“If I chronicled all my negative results during my studies the thesis would have been 20,000 pages instead of 200.” ~ Peter Dudek
There is a tendency for researchers and journals to publish positive studies in both mainstream medicine and alternative medicine. Mlinarić et al. found that the proportion of positive studies had increased since the early 1990s, reaching to about 70 to 86 percent in 2007 among medical research. BMC Complementary and Alternative Medicine also noticed such trend in its own circle and encouraged researchers in the field to published negative findings to “be seen to be honest, self-regulating, and to be striving to identify the treatments and therapies that are truly effective.”
Negative studies are often seen as not useful, unworthy of publishing, and could not be used by academics to advance their career. Thus, the file drawer effect happens where negative studies get tucked away somewhere and would likely be forgotten.
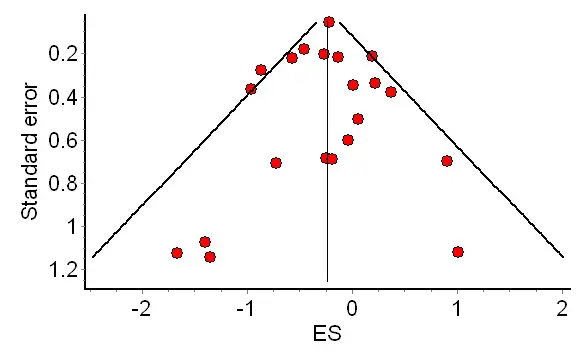
Statisticians sometimes use a funnel plot to check for publication bias in a systematic review or meta-analysis. The horizontal line on the graph indicates the strength of the study, while the vertical line indicates no effect. If a study is positive, it moves toward the right; it is negative, it moves left. Higher quality studies cluster near the top of the funnel and close to the center line. Lower quality studies sink toward the bottom of the graph, and sometimes these studies move toward the right since positive studies are more likely to be published than negative ones.
Related: Should You Get a Massage For Muscle Soreness?
In one example, a 2019 Iranian a meta-analysis and systematic review pooled data from nine studies on the effects of reflexology on premenstrual pain. The researchers found publication bias when they examined the overall effect on pain where five positive studies were near the top and four of them were outside of the funnel. The other four negative studies were also outside of the funnel and moving toward the bottom.
While the researchers concluded that reflexology could alleviate the painful symptoms of menstruation, the effect sizes in the studies were mixed as was the consistency of the outcome, they reported. Otherwise, this seems to be a reasonable conclusion, but there is a little more to the graph than just eyeballing the dots.
Statistician Mark Simmonds from the University of York cautioned about interpreting the funnel plot results. He did a simulation of 10,000 studies where the larger number of studies there, the more likely that it will correctly detect one type of publication bias.
But the type of test a scientist use also matters. When Simmonds compared the three tests used to check for publication bias—Asymmetry Distance, Egger’s, Imbalance—the first one can more accurately detect the bias than the others. This is assuming that all the trials have consistent methodologies. Simmonds said that when there are ten or fewer studies in a meta-analysis and they are funnel-plotted, the results “may be highly misleading.”
Biological plausibility
This is one of the biggest factors that needs to be considered before an experiment is made and money is invested into a research, especially if it pertains to public health. In medicine and healthcare, biological plausibility refers to an explanation of a clinical effects based on established sciences, such as biology, chemistry, and physics. Because reflexology is based on pre-scientific ideas or unproven claims, such as energy channels, acupoints, and zones, the cause and effect explanations of how it works does not validate its effectiveness.
A more plausible explanation for some of the painkilling and mood-altering effects of reflexology or massage could stem from a change of hormone levels in the blood and the brain—such as oxytocin—when a patient is touched, a strong and favorable therapeutic relationship between the patient and caregiver who spends more time listening (which might give reflexology its trust and popularity across cultures), and patients’ expectations and prior experience of an intervention.
How to find the best therapist in reflexology near you

While the claims and narratives of reflexology can sound far-fetched, there is little doubt about its therapeutic benefits, such as alleviating musculoskeletal pain and promoting relaxation like massage therapy. Like looking for a massage therapist who is right for you, considering the following.
Listen to understand you
Part of being a healthcare professional or caregiver is having good quality people skills. It seems like a no-brainer, but research has found that many physicians do not listen to their patients or validate their pain experience. Women are also taken less seriously than men by medical professionals.
You could apply these lessons to finding a massage therapist or reflexologist. Make sure they understand why you came to see them.
Knowledge about the human body based on plausibility
Good reflexologists should have a strong understanding of human physiology, anatomy, and the biopsychosocial model of pain. These are the foundations that should guide treatment, identify potential pathologies, and stay within their scope of practice. This allows proper communication to other healthcare professionals if the reflexologist encounters a medical problem and need to inform the client or patient and his or her medical provider.
Knowledge about the roots of reflexology
There is a social element of reflexology that many cultures worldwide embrace. Perhaps it is an identity or history that they value, which is told in the hands-on work. Thus, acknowledging the roots of reflexology means the practitioner honors the tradition and the culture that brought forth the practice.
Global health expert Clay Jones wrote about the importance of honoring traditions and folk remedies that has been among various cultures for centuries. “Shamanic and traditional beliefs and practices still exist in the world today and are quite prevalent in low and middle income countries,” he wrote when he was a graduate student at Duke Global Health Institute in 2016.
“From Amazon rainforest shamans in Peru to religious healers in Kathmandu to African herbalists, traditional healing practices and beliefs weave into the fabric of a country’s culture. These beliefs and traditions are ingrained in communities and are an important aspect of their health-seeking behaviors, culture and collective psychology.”
It is similar to how pain researchers, physicians, and physiotherapists honor the work of previous scientists in understanding pain, such as Von Frey, Livingston, and Melzack.
Informed consent
Practitioners must give informed consent to clients and patients before the session starts, in addition to a health assessment and history intake. Informed consent means that they have “the right to receive information and ask questions about recommended treatments so that they can make well-considered decisions about care,” according to the American Medical Association.
The College of Massage Therapists of British Columbia states that health care providers “must not provide any health care to an adult without the adult’s consent” other than a few exceptions. (Registered massage therapists in Canada are health care professionals by law so this applies to them.)
For example, you agreed to received a reflexology treatment and the practitioner had informed you that only your feet and ankles will be worked on. Halfway through the session, she moved toward your neck and started to massage your head, face, and neck. That would be a breach of informed consent because you had not agreed to have those areas touched or worked on. Likewise, if the practitioner uses aromatherapy or a balm that you had not requested to be used on you, that also is a breach of informed consent.
Bottom line: Make sure that you are well-informed of what is to be expected during your session. If the practitioner is doing something to you that is not part of what you had agreed with, then let him or her know. Also, you may file a complaint to the city, state, or province if there is a board or regulatory body in your area.
Licensed or certified
Check if your therapist is certified or licensed through their local, state, or province. For example, there is no statewide regulation or mandatory requirement of practicing reflexology in California, but Washington state has certification requirement in the state’s legislature under the umbrella of massage therapy. This ensures not only he or she fulfills the minimum requirement to practice, it means the therapist also passed a background check (usually FBI). You should be able to see the therapist’s license or certificate displayed publicly in the practice.
Like massage therapy, reflexology can be relaxing and just feel good, a way to alleviate stress and pain. Like massage therapy research, however, the quality of reflexology research needs to improve its reporting and reduce its biases while questioning the nature of the treatment and narratives that practitioners tell to their clients and patients.
Based on the evidence so far, it seems that reflexology is a form a social touch where being present with another person—the physical touch, the conversations, etc.—can help alleviate suffering. Practitioners in early civilizations used narratives and stories to connect with the person in pain. They were able to explain their treatment and the symptoms based on the best ideas and tools they had at the time. While the modern understanding of human physiology had much advanced since the Pyramids of Giza were built, the narratives still matter to some people and cultures. Even so, patients and clients still need to be well-informed about what reflexology can and cannot do, based on the best available evidence.
Nick Ng, BA
Nick Ng is the editor of Massage & Fitness Jounal and the managing editor for My Neighborhood News Group.
An alumni from San Diego State University with a bachelor’s degree in graphic communications, Nick had also completed his massage therapy training at International Professional School of Bodywork in San Diego in 2014. In 2021, he earned an associate’s degree in journalism at Palomar College.
When he gets a chance, he enjoys weightlifting at the gym, salsa dancing, and exploring new areas in the Puget Sound area in Washington state.



