A recent cross-sectional study from Duke Integrative Medicine in Durham, North Carolina, found that massage therapy (Swedish style) can alleviate pain among people with knee osteoarthritis. It was better than groups that received light touching or “usual care.” However, the benefits of massage therapy lessened after eight weeks, and by week 52, there was “no significant difference” among all groups.
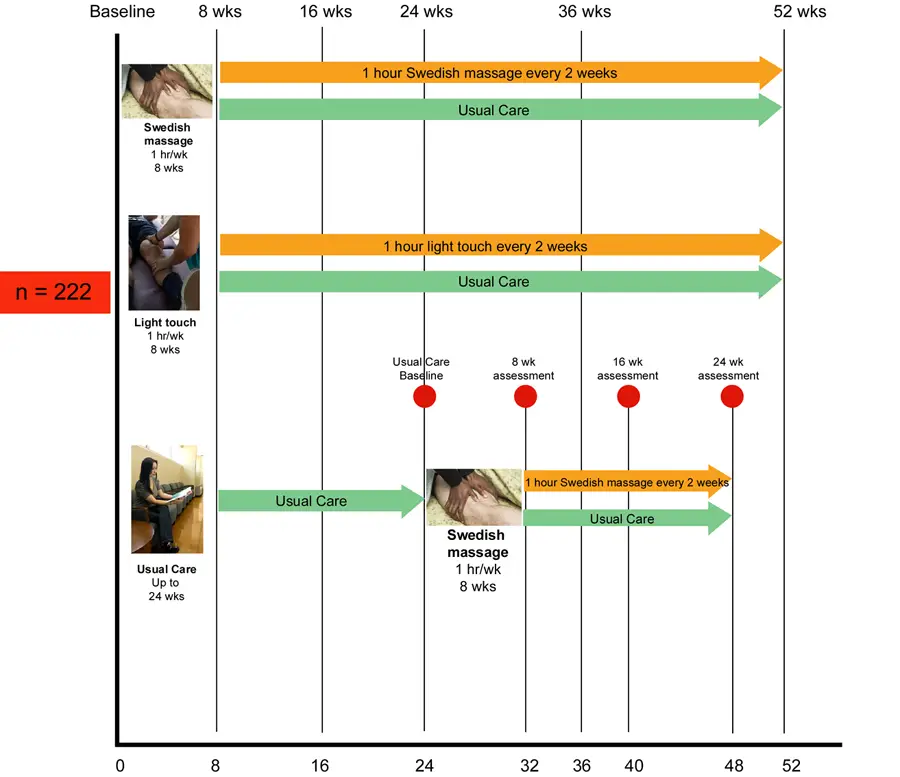
Among 222 eligible subjects who enrolled in the study, they were randomized into three groups for the first eight weeks: massage therapy, light touch, and usual care.
The massage group received one hour of full-body Swedish massage once a week, and the light touch group received touch (but no tissue “manipulation”) in a certain sequence, which involved the therapist placing hands upon a body part.
After eight weeks, the subjects in these two groups were re-assessed for pain and range of motion and were reassigned to one of the following groups: one hour of “maintenance” Swedish massage or light touch (respective to the same group) every two weeks or usual care.
However, the usual care control group ended their care at 24 weeks, and the subjects received the same Swedish massage protocol for eight weeks. After that eight weeks, they were randomly assigned to either one hour of Swedish massage every two weeks or usual care for 16 weeks—up to week 48 of the entire study.
At the end of the study, the dropout rate was eight (about 11%) for the massage group, 25 (about 34%) for the light touch group, and seven (about 9%) for the usual care group. A large number of people dropped out from the light touch group because they reported that they didn’t think there was much benefit from the treatment.
“This study was [a] continuation of a line of research we have done investigating massage for osteoarthritis of the knee,” Dr. Adam Perlman explained to Massage & Fitness Magazine. “Massage is often used by people to treat painful conditions, arthritis being one of those. However, there was very little if any clinical research when we started to inform patients and healthcare providers regarding the safety and efficacy of massage. Contributing to that body of literature and enabling better, more evidence-based decisions that
hopefully leads to relief of suffering and improved quality of life for the multitude of people with chronic pain was the ultimate inspiration.
“They were reassigned to either maintenance massage, maintenance light touch (our ‘placebo’ intervention) or no maintenance in order to investigate if maintenance massage (every other week) would make a difference over the subsequent year,” Perlman said.
When asked why the groups were divided a “maintenance” group and a “usual care” group, Perlman said that getting a massage weekly for a year could be quite costly for most people in the real world.
“We were hoping to show that you could cut back on the frequency,” he said. “Since we don’t know exactly what the subjects did outside of the study over that year, we can’t really say why all the groups improved, but the takeaway is that massage lead to more immediate improvement.”
“We attempted to track things like medication use and determine the cost-effectiveness of massage, but found that difficult,” Perlman continued when asked what could be improved in the study. “Not an improvement necessarily, but a different methodology would be to compare massage to other active interventions. We also need more investigation into the mechanism of massage for osteoarthritis and other conditions.”
Knee osteoarthritis options besides massage therapy
Massage therapy can be costly for many people with knee osteoarthritis, even if it is done biweekly. Dr. Jeffrey Jackson from Zablocki VA Medical Center in Milwaukee, Wisconsin, said that what is not clear from the study is whether weekly Swedish massage might lead to sustained improvement.
“The improvement appears to last for the 8 weeks that weekly massage was being provided; after that, having a massage every other week appears to not be therapeutic,” Jackson said.
He cited a 2017 review of knee osteoarthritis treatment that found two non-pharmacological and non-invasive treatments that show some promising evidence of alleviating pain: weight loss and general exercise.
“A common problem is that trials were either too short or too low quality to provide good evidence of efficacy. This study is a good example of the rigorous approach that needs to be incorporated to obtain strong evidence for benefit from CAM options,” Jackson said.
Limitations of knee osteoarthritis
Perlman and his team mentioned a few limitations that should be considered:
1. Small and somewhat homogeneous sample (mostly female and Caucasian)
2. Difficulty in blinding subjects and massage therapists to the active treatment groups. Thus, it’s likely that the subjects’ bias may have influenced the high dropout rate and results of the light touch group. Bias among massage therapists may have also influenced the quality of the massage or light touch group.
3. The WOMAC scores among the subjects were not validated for clinical significance, which means we don’t really know for certainty if there’s an noticeable difference among the groups.
4. The researchers did not assess for existing chronic diseases or psychological issues that are common among those with chronic pain, such as anxiety and depression.
Also, the data was gathered from one point in time, so a direct cause-and-effect relationship between massage or light touch with knee pain could not be established.
Although massage therapy has short-term benefits, this does not mean that clients or patients in pain should not get a massage. For many people, perhaps a better to way to treat knee osteoarthritic pain is a combination of exercise, massage, medications (if needed), and other lifestyle factors, such as sleep, diet, and having a strong social support. Meanwhile, Perlman and his team suggested that future research in massage therapy should compare the effects of massage therapy and light touch, such as biochemical, immunological, and mechanical.
“The message supported by our previous research and reinforced with this study is that massage is a potentially effective short term strategy in addition to usual care for people with osteoarthritis of the knee who are looking for a non-medication, non-surgical approach to improving their pain and function,” Perlman said. “Our study didn’t investigate the efficacy of massage for other joints and the best
way to maintain the improvement long-term is still unclear.”
Nick Ng, BA
Nick Ng is the editor of Massage & Fitness Jounal and the managing editor for My Neighborhood News Group.
An alumni from San Diego State University with a bachelor’s degree in graphic communications, Nick had also completed his massage therapy training at International Professional School of Bodywork in San Diego in 2014. In 2021, he earned an associate’s degree in journalism at Palomar College.
When he gets a chance, he enjoys weightlifting at the gym, salsa dancing, and exploring new areas in the Puget Sound area in Washington state.



