For decades, many physicians and manual therapists believed osteoarthritis pain was rooted primarily in the joints. However, research in the past 20 years is pointing toward the brain and spinal cord as key players in how pain is felt and processed, including different types of arthritis.
A 2025 review published in Nature Reviews Rheumatology challenges the traditional views of osteoarthritis as mainly a physical condition tied to joint damage and the brain is a passive recipient of nociceptive signals from peripheral nerves.
Researchers from the Feinberg School of Medicine at Northwestern University proposed that long-term activation of pain-sensing nerves can reshape brain function, which helps explain why some patients still feel severe pain even when their joints show only mild damage or after a total joint replacement. The findings may open doors to more personalized treatments.
Led by Dr. Apkar Vania Apkarian, the research team—including Dr. Paulo Branco and Dr. Joana Barroso—identified three steps on how osteoarthritis pain develops:
- Prolonged joint damage—such as wear and tear, changes in joint structure, and long-term inflammation—activates nociceptors (specialized nerve endings that detect harmful stimuli) in the joint.
- Over time, the brain starts to change in response to this pain, which affects how a person feels and experiences the pain. These brain changes also depend on each person’s unique brain structure and previous pain experiences.
- Among many people, these brain changes keep the pain going even after the joint damage is treated or the joint is replaced.
“Our perspective is that pain in osteoarthritis—much like for all other chronic pain conditions—cannot be solely attributed to joint damage or injury,” Branco said in an interview on behalf of Barroso and Apkarian with Massage & Fitness. “Beyond the joint, the intensity and qualities of pain a patient perceives is also shaped by properties of the central nervous system, for example, through sensitization of neurons in both the spinal cord and the brain, which are known to change during continued exposure to pain.”
First, the research team wrote that “negative emotions and moods alone should not be equated with pain, just as injury and nociceptive signals do not inevitably lead to pain. Both nociceptive activity and emotional responses contribute to the pain experience.”
They described chronic pain as a range of ongoing conditions where the nervous system becomes more sensitive to nociceptive signals—either through changes in the body’s pain pathways or through stronger emotional responses in the brain, or both.
These changes in the nervous system can create a “chronic-pain brain state”—through the spinal cord, emotional brain areas (e.g. limbic system), and higher thinking centers (e.g. prefrontal cortex)—shapes how we personally experience pain. This is why pain isn’t just physical; it also has emotional, mental, and motivational effects.
Over time, chronic pain can turn into a kind of learning process that becomes unhealthy, the researchers wrote. A person can lose their connection to actual threats in the environment and start to feel like a part of the person’s identity. This can make emotional distress worse and make it harder for someone to manage or think clearly about their pain.
The brain and chronic pain, a brief review
The researchers highlighted three different “domains” of the pain experience and added one mechanism that gives us the pain experience. This is an expansion of the “three dimensions of pain” proposed by Dr. Ronald Melzack and Dr. Kenneth Casey in 1968 in their book The Skin Senses.
- Sensory–discriminative domain, which helps us detect where pain is coming from, how strong it is, and what kind of pain it feels like.
- Affective–motivational domain, which helps us emotionally react to pain, motivates us to change our behavior, and helps us learn to avoid harmful situations through positive and negative reinforcement.
- Cognitive–evaluative domain, which allows us to combine what we sense and feel emotionally.
- Descending modulation, which allows the brain to influence and control nociceptive signals traveling through the spinal cord. This process can increase or decrease the amount of pain we feel.
The three domains’ principles are based on the gate control theory of pain and the neuromatrix theory of pain.

“We know that the brain controls the pain you feel in several ways,” Branco said. “For instance, the brain can ‘talk’ with the spinal cord and inhibit the transmission of body signals to the brain. The brain can also amplify or diminish the salience of these signals based on the environment.”
Branco gave an example where amplifying pain perception is important for survival, such as touching a stove. “Not only do you identify a burning sensation on your hand, but you also sense it as an aversive, highly unpleasant experience,” he said. “It should come naturally then that, from this viewpoint, pain is inherently subjective, where the brain constructs your pain experience based on several brain processes. Some of which will change given your past experiences, your environment, your genetics, and others.”
Here’s how the four brain regions and systems work together.
Sensory-discriminative domain
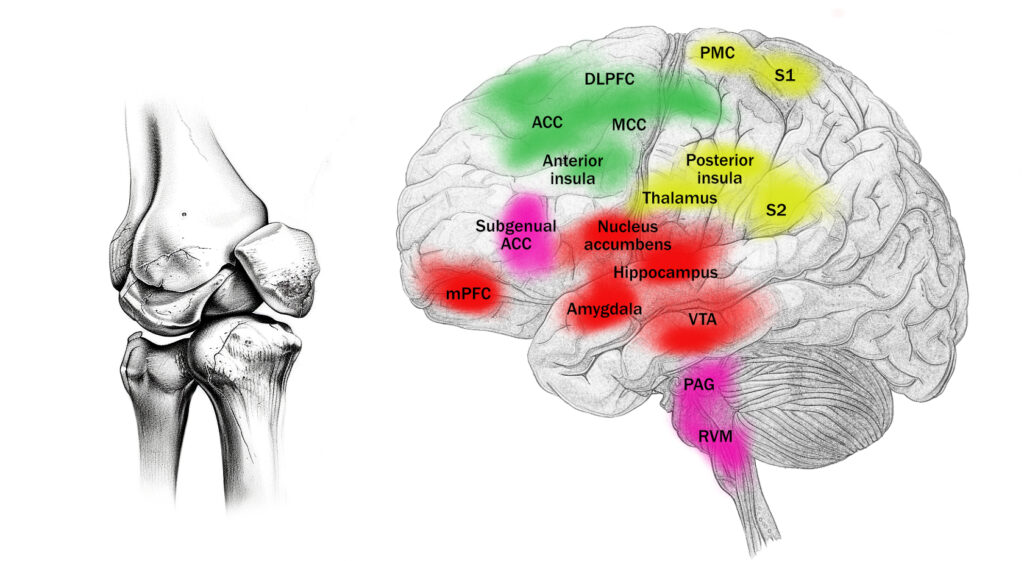
Apkarian, Barroso, and Branco described the sensory–discriminative domain as a link of brain pathways that carry nociceptive signals from the peripheral nerves to the brain. These areas include the thalamus, the primary and secondary sensory cortices, the primary motor cortex, and the posterior insula.
Together, these brain regions help you know where the pain is coming from, how strong it is, and what kind of pain it is. While these systems have mostly been seen as just receiving and interpreting nociception, research shows that chronic osteoarthritis pain causes changes in how these brain areas adapt and are structured.
Among these regions, the thalamus has been one of the most studied brain parts in osteoarthritis patients. Brain imaging studies show that people with chronic osteoarthritis pain have less grey matter in the thalamus and lower levels of a brain chemical called N-acetyl aspartate, which is linked to healthy nerve function.
These people also have reduced blood flow in the thalamus, which suggests it may not be working properly. Therefore, abnormal thalamus activity may result from the brain reacting to constant nociceptive signals. In fact, the more pain a person feels, the more strongly the thalamus appears to be connected with other pain-related brain areas. This pattern becomes even stronger after the person experiences increased pain, such as after moving or a physical activity.
“Given the role of the thalamus as a relay of nociception, these abnormalities are likely to act as a first step in supraspinal amplification of the nociceptive barrage as the disease progresses, and this amplified signal is then propagated to other systems,” the researchers wrote.
After reaching the thalamus, nociceptive signals travel to the brain’s sensory cortices where the brain processes how strong the pain is and where it’s located. Just like with the thalamus, people with osteoarthritis often show shrinkage in these sensory areas, and smaller volumes are linked to lower pain tolerance. This suggests that the brain may become more sensitive to pain over time.
The researchers added that the primary motor cortex shows changes in osteoarthritis, likely due to reduced movement and long-term changes in how the body adapts to pain. This includes brain shrinkage, increased nerve activity, and changes to the brain’s “map” of body movement. While these changes may not be caused by pain alone, they may reflect how the body and brain adjust to living with the condition.
“Structural and functional changes in key regions such as the thalamus, sensory and motor cortex suggest that persistent nociceptive input leads to widespread neural reorganization,” the researchers wrote. “These adaptations might, in turn, contribute to increased pain sensitivity and altered pain thresholds, heightening the pain experience.”
Affective–motivational domain
In the brain’s limbic system, the mesocorticolimbic network—which includes the mesolimbic system (ventral tegmental area and nucleus accumbens) and the corticolimbic system (amygdala, hippocampus, and ventromedial prefrontal cortex)—plays a key role in the development of chronic pain. Apkarian, Barroso, and Branco wrote that as pain becomes long-lasting, the connections in these brain circuits change, especially those that deal with the emotional side of pain.
“The vmPFC [ventromedial prefrontal cortex], a key structure of the mesocorticolimbic system, also shows a decrease in grey matter volume in osteoarthritis,” they wrote. “Importantly, the vmPFC and its extended circuitry is massively engaged when patients are asked to track their own ongoing pain in real time, but not when they track responses to experimental [acute] painful stimuli.”
The mesocorticolimbic system provides a “learning signal that guides adaptive behaviour through aversive and reward signalling, thus priming the system to shift its behaviour to cope with pain,” the researchers wrote.
While this behavior is helpful right after an injury, if the brain doesn’t return to normal, it can lead to ongoing pain that doesn’t serve a protective purpose anymore, they added.
Studies of osteoarthritis patients show that brain regions, such as the nucleus accumbens, hippocampus, and amygdala, shrink and have lower blood flow among people with osteoarthritis.
“Pain has been associated with increased activity in the amygdala, and both amygdala and hippocampal responses to experimental painful stimuli decrease after intake of NSAIDs [nonsteroidal anti-inflammatory drugs], hinting that these structures might encode nociception,” Apakarian, Barroso, and Branco wrote.
However, they pointed out that activity in the amygdala and hippocampus is also linked to how much pain a person feels at any moment. However, this link also seems to involve how anxious the person feels, suggesting that these brain areas may be more involved in the emotional and motivational side of pain—like how the brain reacts to and evaluates pain—rather than processing the actual nociceptive signals themselves.
Cognitive–evaluative domain
Higher functions of the brain, such as the insula and anterior cingulate cortex (ACC), are connected to brain regions that handle emotions, sensory input, and pain control. Apkarian, Barroso, and Branco wrote that among many osteoarthritis patients, the insula tends to be smaller in size compared to healthy people, and this shrinkage has been linked to “ the continued stress and ongoing burden of the disease.”
While the insula shows less blood flow at rest, it also shows more spontaneous brain activity, which might reflect its overactive response to ongoing pain. In people with knee osteoarthritis, the anterior insula shows a loss of “hubness” and “degree.”
They described hubness as the role of a brain region as a “central hub or a key connector that facilitates communication between different brain regions.” Degree is the number of direct connections a region has with other brain areas.
“A loss in both ‘hubness’ and ‘degree’ means that the insula is less connected and has a compromised role in overall brain communication, which is consistent with other findings in [osteoarthritis] showing disruptions in the functional connectivity between the insula and the medial thalamus, the prefrontal cortex and several other cognitive and affective brain regions,” they wrote.
Regarding the ACC, Apakarian, Barroso, and Branco wrote that joint pain in osteoarthritis patients activates the ACC, but this doesn’t happen with other types of pain, such as thermal pain. This suggests that ongoing osteoarthritis pain is processed differently by the brain, they concluded. Also, they pointed out that patients who were taught to cope with their pain had less pain and lower ACC activity.
Since the ACC can influence how nociceptive signals move up the spinal cord, it’s likely involved in controlling how pain is perceived from the top down.
Descending modulation
Descending modulation is the central nervous system’s ability to regulate nociceptive input via pathways that originate in the brain and project downward to the spinal cord. These pathways, which include the periaqueductal gray (PAG), rostroventral medulla (RVM), and dorsolateral pontine tegmentum, can amplify or reduce activities in the dorsal horn neurons that process incoming nociceptive signals.
This modulation is influenced by various factors, including cognitive and emotional states, and plays a critical role in shaping the final pain experience, contributing to phenomena such as placebo analgesia and chronic pain sensitization.
Apkarian, Barroso, and Branco described the brain receives information from various brain regions that involve thinking and regulating emotions and stress, such as the ACC, the ventromedial prefrontal cortex, the hypothalamus, and the amygdala. These connections allow thoughts, feelings, and motivations to influence how pain signals are processed in the spinal cord.
The researchers highlighted that brain scans of people with osteoarthritis show that this descending modulation doesn’t work normally. Compared to people with no pain, those with osteoarthritis have lower blood flow in the PAG and more brain activity when painful pressure is applied to their affected joints. Higher responses in the RVM and cingulate cortex are also found in people with osteoarthritis who report these nerve-like pain symptoms.
They noted that such abnormal RVM activity before surgery can predict who will go on to have long-term pain after a joint replacement. “Abnormal RVM activity was captured before surgery, it does not reflect surgical consequences and, thus, implies that the brain is either pre-emptively sensitized to incoming nociceptive inputs, possibly due to a chronic state of nociceptive facilitation, or primed to amplify these signals,” the researchers wrote.
However, they cited a 2018 study that found exercise (in the forms of stationary cycling, tai chi, and Baduanjin—a form of qigong) can affect descending modulation positively by changing the brain’s pain control and reward systems, as well as levels of inflammation in the blood.
Some studies on osteoarthritis have found that when people experience pain relief with “manipulating expectations or learning pain-coping strategies,” they wrote. “Together, these findings suggest that sensory, affective and cognitive systems can exert control over nociception through descending modulation, and that this modulatory system is also likely to be impaired in a subset of patients with [osteoarthritis].”
Putting the domain model to use
Branco said that the their goal is to emphasize that the pain experience is not solely determined by nociception, but rather “emerges from a complex interplay of factors—from peripheral and central sensitization to various brain processes” in the domains. Still, there are many questions left unanswered.
“For instance, how interdependent are these parameters, and how addressing one of these parameters changes the others?” Branco said. “If we treat the peripheral, nociceptive component, how much of the cognitive-evaluative component are we changing, and vice-versa? This has direct clinical implications, such as determining whether a patient will benefit more from an NSAID, psychotherapy, or even physical therapy targeting kinesiophobia [fear of movement], or whether another patient might respond better to peripheral nerve modulation or different combinations of the above.”
He asked if there are additional parameters that should be incorporated into the model, such as genetic or psychosocial factors.
“From a clinical viewpoint, if we can quantify all properties of this model in patients, could we predict the efficacy of a given treatment? Or help clinicians plan personalized treatment strategies based on the most abnormal parameters?” Branco said. “And finally, how can we measure brain properties in ways that are accessible, affordable, and practical for clinicians and therapists, without requiring advanced equipment or specialized expertise? These are all critical questions that future research must address.
“Ultimately, our ongoing work seeks to develop a way to identify, on an individual level, which systems are contributing the most to the experienced pain, with the goal of optimizing chronic pain treatments for each patient.”
A model for osteoarthritis pain
Based on these domains, Apkarian, Barroso, and Branco proposed a model that shows how each person with osteoarthritis pain can have different degrees of influences from different domains and mechanisms. Thus, individualized treatments are warranted for each unique case.
They gave examples where Patient A may benefit from NSAIDS, joint injections or total joint replacement if their osteoarthritis pain stems primarily from nociceptors in the peripheral nerves. However, Patient B may benefit from spinal cord stimulation or transcutaneous electrical nerve stimulation (TENS) if their primary cause is peripheral sensitization or spinal sensitization.
“This approach would enable testing of the influence of various factors on pain perception and explore individual differences by assuming that these components vary among [osteoarthritis] patients. Consequently, this variability might be linked to distinct clinical presentations and responses to treatments,” the researchers wrote.
These personal differences may help explain why some people respond well to typical treatments, while others—like those who still feel pain after a joint replacement—do not get relief.
Branco said that chronic pain must be understood from multiple perspectives, “not only through the traditional medical lens that focuses on identifying and fixing the injury, but also through a broader biopsychosocial framework.”
“This perspective recognizes that injury-related factors are only one part of a much larger puzzle,” Branco said. “To effectively treat chronic osteoarthritis pain—and chronic pain more generally—we must first deepen our understanding of the diverse factors that shape the pain experience, and we must approach treatment from a multidisciplinary standpoint, while at the same time recognizing that each patient is unique and likely requires tailored treatment.”
Nick Ng, BA
Nick Ng is the editor of Massage & Fitness Jounal and the managing editor for My Neighborhood News Group.
An alumni from San Diego State University with a bachelor’s degree in graphic communications, Nick had also completed his massage therapy training at International Professional School of Bodywork in San Diego in 2014. In 2021, he earned an associate’s degree in journalism at Palomar College.
When he gets a chance, he enjoys weightlifting at the gym, salsa dancing, and exploring new areas in the Puget Sound area in Washington state.
