Although we still have a lot to learn about how muscles contract, we do understand the basics of how the nervous system initiates a series of actions that contract a muscle.
What about muscle movements that we don’t consciously decide to make, like breathing, digestion, and heartbeats? And what about muscle spasms? The secret behind all these activities is muscle shortening or “contraction.” Let’s begin with a clear understanding of how muscle tissues work and how massage therapy can affect it.
Skeletal muscle contraction
Like other vertebrates, there are three kinds of muscle:
- Skeletal: These are the only muscles that we can contract consciously, and they are the type that most (not all) massage therapists intend to treat.
- Cardiac: Stripey muscles that contract involuntarily in your heart.
- Smooth: Muscles that don’t have stripes and contract involuntarily in your blood vessels and intestines.
Types of muscle contraction
Skeletal muscles undergo three different kinds of contraction: Concentric, eccentric, and isometric.
Visualize a muscle at rest. It has a certain length and a degree of tension, and they’re going to remain more or less the same until force is applied to it. When that happens, the muscle can resist by changing its tension or its length.
The Greek and Latin names for the different kinds of contractions describe what happens when muscles work. Isotonic contractions, from the Greek words “iso” + “tonic” meaning “same/equal” + “tension.” In isotonic contractions, the muscle tension remains the same, while the length of the muscle changes. The muscle can lengthen (eccentric contraction) or shorten (concentric contraction).
Isometric contractions, from the Greek words “iso” + “metron” meaning “same/equal” + “measure.”
In isometric contractions, the muscle length remains the same while the muscle tension changes. Let’s look at how that works in real-life examples.
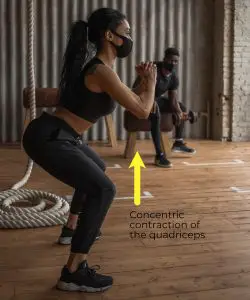
Concentric contraction
When you lift something, the muscles that you are flexing, such as your biceps, are shortening in length. This is an example of concentric contractions. Examples include a client experiencing pain while closing their jaw or flexing an arm or leg muscle.
Eccentric contraction
Eccentric contraction, which is a second kind of isotonic contraction, is when the force on the muscles is stronger than the muscle itself. The muscles are moving in the opposite direction of the muscle’s direction of contraction.

When you extend your biceps because you’re lowering something, or because what you’re trying to lift is too heavy to continue flexing, you’re doing eccentric contractions. Lifting weights involves both kinds of isotonic contractions.
Isometric contraction
Isometric contraction is when force is applied to a muscle, the muscle is contracting yet remains the same length. Examples include holding position during sports and dance motions or holding a barbell over your head for a few seconds.
How do muscles contract?
The sliding filament theory, with cross-bridge cycling as a molecular mechanism, is widely accepted as the best current representation of how muscles contract. Muscle contraction is understood as a cycle of smaller contractions, repeating at the molecular level.
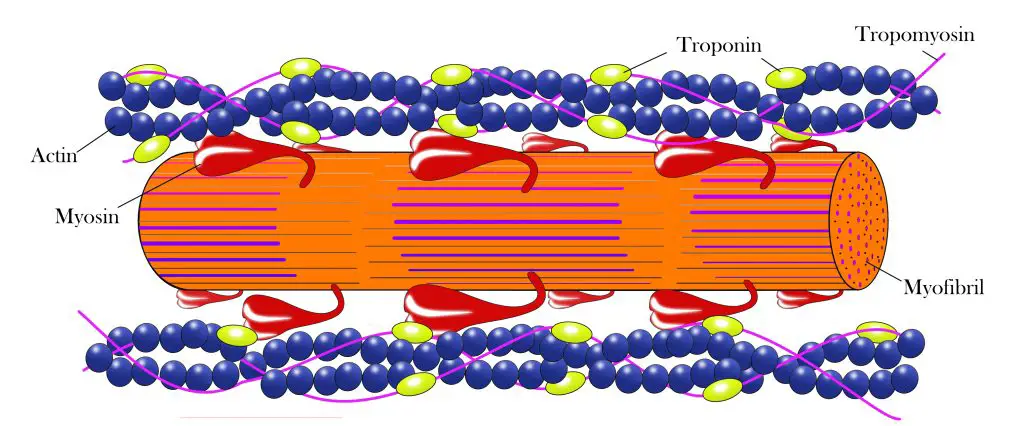
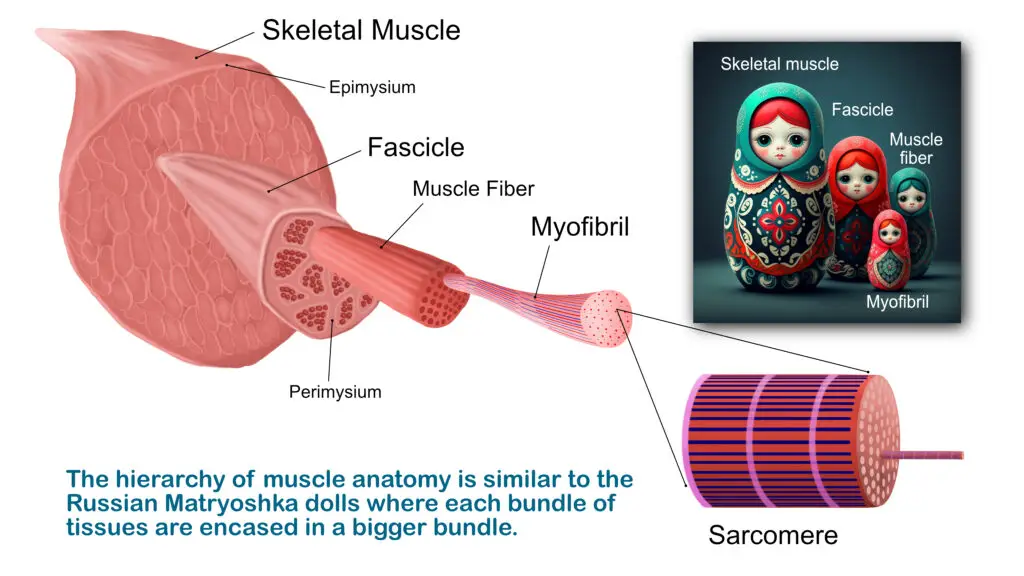
Sarcomeres, which are the basic structure of muscle fibers, contain thin and thick filaments. The thin actin filaments and the thick myosin filaments overlap each other, allowing them to slide past each other to create the contraction.
This sliding causes the sarcomere to shorten, which causes the muscle to shorten. But what makes the filaments slide past each other? That’s where cross-bridge cycling at the molecular level comes in.
The cycle starts when a nerve impulse stimulates muscle fibers, and calcium ions are released. These calcium ions bind to the actin (thin) filaments, causing the previously bound myosin binding sites to become available. They still contain adenosine diphosphate (ADP) and phosphate molecules from previous contractions, which they release.
The release of ADP and phosphate free up the binding sites, which bind once again to the actin filaments. The “heads” of the myosin molecules then slide in the direction of contraction, and the actin bound to them are pulled along.
Adenosine triphosphate (ATP) then binds to the myosin heads, breaking their connection with the actin until the next cycle. The myosin breaks ATP down into ADP and phosphate and is ready for the next cycle.
Muscle “release”— what does it really mean?
The word “release” can be confusing when we’re talking about massage’s effects on tissues. When a client uses it, they are often describing what their experience feels like to them, like muscle soreness or tightness. What’s really going on in our bodies can often feel like something very different than what is actually taking place.
Physical therapist and educator Walt Fritz in Rochester, New York, takes a different approach to describe release. He treats muscle tension dysphonia and dysphagia (voice and swallowing disorders) with a style of manual therapy bearing the old name of “myofascial release.”
“When my patient uses it, I allow their perspective without judgment, though I may ask them what they mean by the statement,” Fritz said. “However, in a professional vernacular, it needs to be explained and validated. We are all too familiar with the sloppiness of the term or the coded way in which it’s spoken.”
He said this term was attached to a style of manual therapy in the 1800s when there was much less understanding of how bodies work than there is today. However, the old explanations remain widespread in the massage therapy community.
Muscle cells undergo metabolism as any cell does, taking in oxygen and nutrients, and producing water, carbon dioxide, and ATP. Under certain exercise conditions, muscles can produce lactate and pyruvate as a byproduct of breaking down glucose. These metabolic processes are all reasonably well understood and are a crucial part of normal muscle function.
However, there is a persistent belief among some massage therapists that massage causes muscles to “release toxins.” There’s no evidence and no scientific basis to believe that massage can cause individual muscle cells to “release toxins.” Some massage schools still teaches it, despite the harm of misleading clients and communicating to other healthcare professionals.
For therapists
Think back to your muscle anatomy and physiology class. Remember when you learned that a skeletal muscle has an origin and an insertion. Although the insertion may move closer to the origin when the muscle is flexed, the actual msucle structure does not change.
When the insertion moves away from the origin during muscle extension, the distance between them hasn’t changed from the original position. The origin and the insertion are a certain distance away from each other, and the muscle spans that distance—so there’s really no change in length in the muscle when it’s returned to full extension.
Since length and tension are the two things that can vary in muscle contractions, neither stretching nor massage can change the actual length of the muscles. The change in tension in a healthy muscle can be experienced as “lengthening” the muscle.
Related: Can your massage therapist stretch your fascia?
Summary
Skeletal muscle contracts in three ways:
- Isotonic (“same tension”) contractions, where the muscle shortens (concentric) or extends back to its relaxed length (eccentric).
- Isometric (“same measure”) contractions, where the muscle length doesn’t change.
- The cross-bridge model describes how muscle contraction and relaxation occur, as a result of molecular interactions among actin and myosin filaments in muscle fibers.
Massage therapy does not lengthen muscles, although the change in perception of tension may be experienced as lengthening. Muscle cells undergo the same metabolic processes as other cells do, and they have similar inputs and outputs for cellular respiration.
Therefore, there’s no evidence or plausibility that massage causes muscles to release toxins. On its own merits, massage therapy can be an important part of self-care, wellness, and fitness and can contribute to a program of healthy exercise.
First published May 28, 2022. Updated May 9, 2026.